
Creator: Alisha G C
Teclistamab is a first-in-class bispecific antibody concentrating on B-cell maturation antigen (BCMA) and CD3 that has considerably superior the therapy of relapsed or refractory a number of myeloma (RRMM). By concurrently binding malignant plasma cells and cytotoxic T lymphocytes, Teclistamab redirects endogenous T cells to remove BCMA-expressing tumor cells by main histocompatibility complicated (MHC)–unbiased immune activation. This mechanism bypasses limitations related to standard chemotherapy and antigen-restricted immunotherapies. Medical trials have demonstrated substantial response charges in closely pretreated a number of myeloma sufferers, together with people refractory to proteasome inhibitors, immunomodulatory medicine, and anti-CD38 monoclonal antibodies. Nonetheless, therapeutic resistance pushed by antigen downregulation, T-cell exhaustion, and tumor microenvironment–mediated immune suppression stays a big problem. This evaluate supplies an in-depth evaluation of Teclistamab’s molecular structure, immunologic mechanism of motion, pharmacokinetics, medical efficacy, resistance pathways, and rising methods designed to boost therapeutic sturdiness.
Teclistamab is a humanized bispecific IgG4 monoclonal antibody engineered to concurrently bind:
This dual-binding configuration permits direct immune synapse formation between T cells and tumor cells, triggering focused cytotoxic responses.
Not like smaller bispecific T-cell engager (BiTE) molecules reminiscent of Blinatumomab, Teclistamab retains a modified Fc area, which improves structural stability and pharmacokinetic properties whereas minimizing undesirable immune activation.
Key structural traits embrace:
Full-length IgG-based bispecific antibody structure
Engineered Fc area with decreased Fcγ receptor binding
Enhanced serum half-life in contrast with Fc-less bispecific antibodies
Functionality for subcutaneous administration
This design permits sustained therapeutic publicity whereas lowering the necessity for steady infusion.
B-cell maturation antigen (BCMA, also called TNFRSF17) is a transmembrane receptor belonging to the tumor necrosis issue receptor (TNFR) superfamily. It’s expressed totally on:
BCMA performs a central function in plasma cell survival by binding the ligands:
Upon ligand engagement, BCMA prompts intracellular signaling pathways that promote plasma cell proliferation and resistance to apoptosis.
Main downstream pathways embrace:
These pathways assist the survival and enlargement of myeloma cells throughout the bone marrow microenvironment.
From a therapeutic perspective, BCMA represents a super immunotherapy goal as a result of it reveals:
Excessive expression in a number of myeloma cells
Minimal expression in non-plasma cell tissues
Important function in plasma cell survival signaling
These properties permit selective concentrating on of malignant plasma cells whereas limiting off-target toxicity.
The second useful arm of Teclistamab binds CD3ε, a vital part of the T-cell receptor (TCR) complicated.
The CD3 complicated consists of a number of subunits:
CD3γ
CD3δ
CD3ε
CD3ζ homodimer
The CD3ζ chains comprise immunoreceptor tyrosine-based activation motifs (ITAMs) that provoke intracellular signaling following T-cell receptor engagement.
When Teclistamab binds CD3ε:
Polyclonal T cells are recruited to tumor cells
T-cell receptor clustering happens
Intracellular signaling pathways are activated
Importantly, this course of happens independently of antigen presentation, permitting T cells to remove tumor cells even when main histocompatibility complicated (MHC) expression is decreased or absent.
Teclistamab accommodates a modified IgG4 Fc area designed to optimize pharmacokinetic and security profiles.
Key Fc modifications present:
Diminished binding to Fcγ receptors
Decreased antibody-dependent mobile cytotoxicity (ADCC)
Diminished complement activation
Prolonged serum half-life (~3–4 days)
These options allow intermittent subcutaneous dosing quite than steady intravenous infusion.
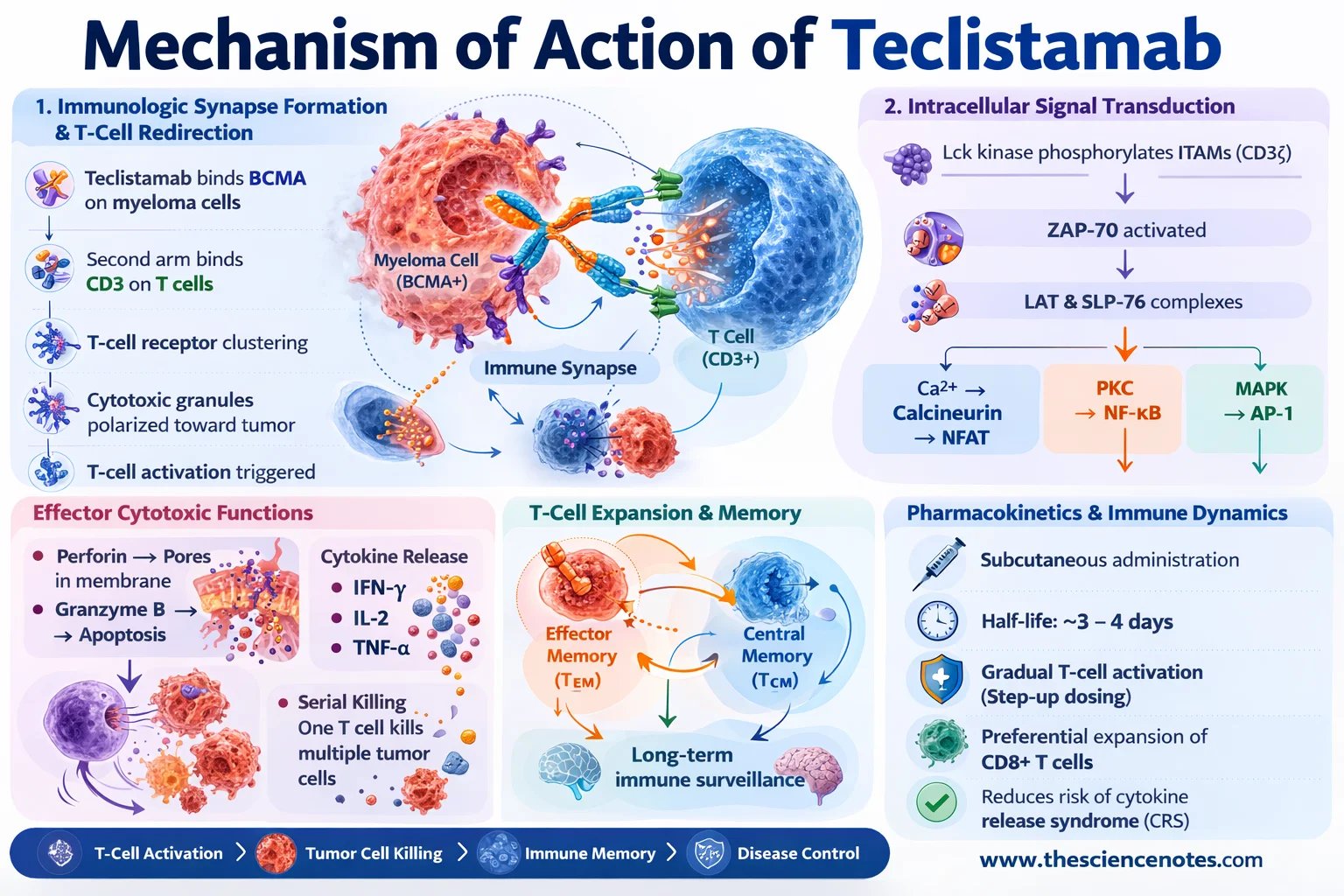
1. Immunologic Synapse Formation and T-Cell Redirection
Teclistamab capabilities by bodily linking CD3-positive T cells to BCMA-expressing myeloma cells, thereby forming a useful cytotoxic immune synapse.
The method includes a number of sequential steps:
Teclistamab binds BCMA on malignant plasma cells.
The second binding arm engages CD3 on T cells.
Shut mobile proximity induces T-cell receptor clustering.
Cytotoxic granules are polarized towards the tumor cell interface.
This synthetic synapse mimics physiological immune cell interactions and triggers T-cell activation.
Intracellular Sign Transduction
Following CD3 engagement, a cascade of intracellular signaling occasions happens:
Lck kinase phosphorylates ITAMs on CD3ζ chains
ZAP-70 is recruited and activated
Adaptor proteins together with LAT and SLP-76 assemble signaling complexes
Downstream signaling pathways are subsequently activated:
Calcium–calcineurin signaling → NFAT activation
Protein kinase C signaling → NF-κB activation
MAP kinase cascade → AP-1 transcriptional activation
Collectively, these transcriptional applications drive T-cell activation, proliferation, and cytotoxic exercise.
Effector Cytotoxic Capabilities
Activated T cells remove tumor cells by a number of mechanisms:
Perforin–Granzyme Cytotoxicity
Perforin types pores in tumor cell membranes, permitting granzyme B to enter and set off apoptosis.
Cytokine Launch
Activated T cells launch inflammatory cytokines reminiscent of:
These cytokines improve immune activation and recruit further immune cells.
Serial Killing
A single activated T cell can disengage and sequentially destroy a number of tumor cells.
2. T-Cell Enlargement and Immune Reminiscence
Along with quick cytotoxic results, Teclistamab promotes enlargement of T-cell populations together with:
These reminiscence populations might contribute to long-term immune surveillance and sustained illness management.
Teclistamab demonstrates favorable pharmacokinetic properties because of its IgG-based construction.
Essential traits embrace:
Subcutaneous administration
Half-life of roughly 3–4 days
Gradual T-cell activation with step-up dosing
Preferential enlargement of CD8+ cytotoxic T cells
Step-up dosing protocols are applied to cut back the danger of cytokine launch syndrome.
The MajesTEC-1 section I/II trial evaluated Teclistamab in sufferers with closely pretreated relapsed or refractory a number of myeloma.
Members had beforehand acquired a number of remedy lessons together with:
Key medical outcomes included:
Total response charge (ORR): ~63%
Full response or higher: ~39%
Median period of response: ~18 months
These outcomes exhibit robust exercise in sufferers with in any other case restricted therapy choices.
Regardless of its therapeutic efficacy, Teclistamab is related to a number of immune-related opposed results.
Cytokine Launch Syndrome (CRS)
CRS is the most typical toxicity and happens because of fast immune activation.
Signs might embrace:
Most instances are grade 1–2 and manageable with supportive remedy or IL-6 blockade.
Infections
Teclistamab might scale back regular plasma cells, resulting in:
Sufferers might require immunoglobulin alternative remedy.
Neurotoxicity
Immune effector cell–related neurotoxicity syndrome (ICANS) might happen, although much less often than with CAR-T remedy.
Signs can embrace:
Confusion
Aphasia
Seizures (uncommon)
1. BCMA Antigen Loss or Downregulation
Tumor cells might evade immune concentrating on by lowering BCMA expression by:
Lack of floor antigen reduces antibody binding and T-cell recruitment.
2. T-Cell Exhaustion
Power immune stimulation might result in dysfunctional T cells characterised by:
Upregulation of inhibitory receptors (PD-1, TIM-3, LAG-3)
Diminished cytokine manufacturing
Decreased cytotoxic capability
3. Immunosuppressive Tumor Microenvironment
The bone marrow microenvironment of a number of myeloma accommodates a number of suppressive immune parts:
Regulatory T cells (Tregs)
Myeloid-derived suppressor cells (MDSCs)
Immunosuppressive cytokines reminiscent of IL-10 and TGF-β
These components impair efficient T-cell responses.
A number of therapeutic methods are beneath investigation.
Twin-Goal Bispecific Antibodies
Focusing on further plasma cell antigens might scale back antigen escape.
Examples embrace:
Immune Checkpoint Inhibition
Combining Teclistamab with checkpoint inhibitors might restore exhausted T cells.
Potential combos embrace:
Anti-PD-1 antibodies
Anti-PD-L1 therapies
Enhancing T-Cell Health
Methods to enhance T-cell persistence embrace:
Each Teclistamab and CAR-T therapies goal BCMA however differ of their method.
Teclistamab
Off-the-shelf antibody remedy
No genetic modification required
Subcutaneous administration
CAR-T Remedy
Requires genetic engineering of affected person T cells
Personalised manufacturing course of
Probably longer-lasting responses
Every remedy presents distinctive benefits relying on medical circumstances.
Teclistamab represents a significant development within the immunotherapy of a number of myeloma by enabling potent BCMA-directed T-cell redirection. Its bispecific antibody design permits efficient tumor killing unbiased of antigen presentation whereas sustaining favorable pharmacokinetic properties. Though challenges reminiscent of antigen escape, T-cell exhaustion, and immunosuppressive microenvironments stay, ongoing analysis into mixture therapies and next-generation bispecific antibodies holds important promise. Continued integration of molecular biology, immunology, and medical innovation shall be important for optimizing Teclistamab-based therapies and reaching sturdy remissions in a number of myeloma.
Q1. What’s Teclistamab?
Teclistamab is a bispecific antibody that targets BCMA on a number of myeloma cells and CD3 on T cells, enabling immune-mediated tumor killing.
Q2. Why is BCMA an vital goal in a number of myeloma?
BCMA is very expressed on malignant plasma cells and performs an important function in plasma cell survival signaling.
Q3. What are the principle unintended effects of Teclistamab?
Frequent unintended effects embrace cytokine launch syndrome, infections, and occasional neurotoxicity.
This autumn. How does Teclistamab differ from CAR-T remedy?
Teclistamab redirects current T cells utilizing an antibody, whereas CAR-T remedy includes genetically modifying affected person T cells.
Q5. What causes resistance to Teclistamab?
Resistance might come up from BCMA antigen loss, T-cell exhaustion, or immunosuppressive components throughout the tumor microenvironment.